

Childhood depression is different from the typical everyday unhappiness that occurs as a part of everyday life. Sadness is a universal human emotion which does not typically signify depression. When sadness becomes pervasive and interferes with social activities, interests, schoolwork, or family life, it often indicates depression.
Youth who have a family history of depression, those who have undergone major life stressors or trauma, and those who engage in screen media excessively are at heightened risk of developing depression. Depression is an increasingly common and impairing condition among children and adolescents. Traditionally, 2% of children and 4% of adolescents suffer from depression at any given time. However, rates of depression have nearly doubled in recent years. Mental Health America (MHA)’s 2022 report found that 15% of Connecticut teens suffered a major depressive episode in the past year.
Depression can cause serious impairment including school failure, social isolation, family conflict and developmental stagnation. Persistent depression puts youth at an elevated risk of developing substance misuse, self-harming, eating disorders, school failure and dropout, marked changes in peer group and suicide. Suicide among adolescents have increased significantly in recent years and is now second only to car accidents among leading causes of adolescent death in Connecticut.
Early identification of adolescent depression is essential to timely engagement in effective treatment. Treatment typically includes behavioral activation or cognitive behavioral therapy. More serious cases often require the addition of medication, usually selective serotonin reuptake inhibitors (SSRIs). Parents must be active participants to motivate their children to engage in treatment and follow recommendations. Treatment may also require assistance to restore academic success, encouragement of social activity and participation in school or community activities, and family therapy to improve support and relationships. Suicidal thoughts and behavior typically warrant emergency mental health evaluation and care. Youth who suffer from depression are at higher risk to develop bipolar disorder, although this is atypical. Youth with depression require regular monitoring by their primary care providers. Mild to moderate depression typically has a good prognosis in adolescence as long as it is properly addressed. More severe depression often requires greater care which may include long-term counseling and/or medication, intensive home-based or outpatient treatments, or inpatient hospitalization. Finding appropriate care can be challenging. MHA’s 2022 report ranked Connecticut 41 out of the 50 states in terms of youth access to treatment for depression, one of the hardest states to find care. Identifying and treating depression effectively can be challenging, but pediatricians can effectively do so, preventing significant harm and suffering to their patients using the guidelines below.
Guidelines for Diagnosis
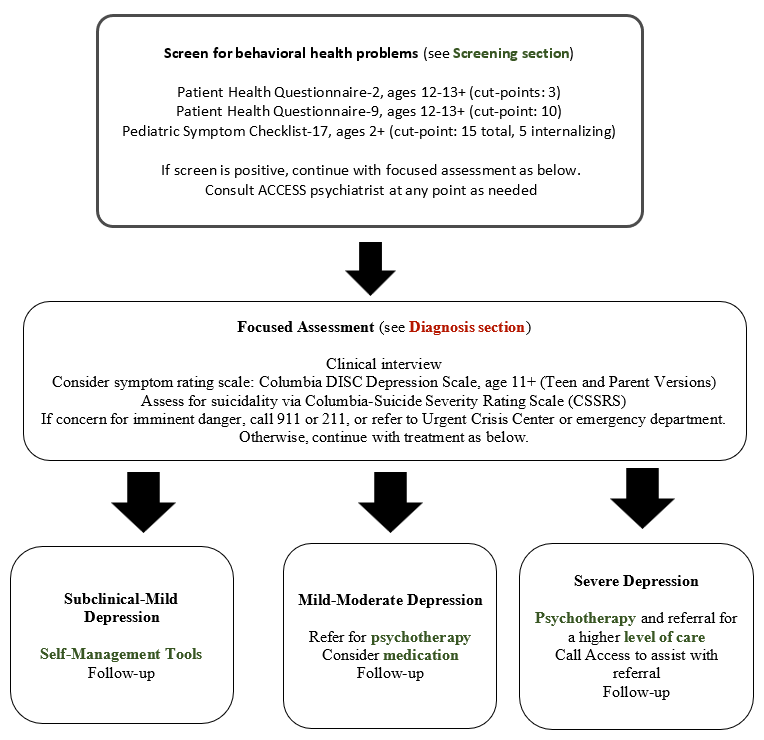
Guidelines for Screening and Assessment
The purpose of the PHQ-2 is to screen for depression in a “first-step” approach. It is accepted as an initial screening instrument for depression in all age groups. The PHQ-2 includes the first two items of the PHQ-9.
If depression is identified by the PHQ-2, completion of the PHQ-9/ PSC-17 and a clinical interview are recommended.
PHQs – https://www.phqscreeners.com/
PSC-17 – https://www.massgeneral.org/assets/mgh/pdf/psychiatry/psc/psc-17-english.pdf
Diagnosis
The list below outlines possible signs of depression. If a child is struggling with any combination of these symptoms for more than two weeks, a mental health professional should be contacted.
Diagnosis
Major Depressive Disorder
DSM Criteria
two weeks of a persistent change in mood that is either depressed or irritable, or persistent loss of interest or anhedonia, accompanied by at least 3 of the following symptoms of a major depressive episode, present most days:
Additional Symptoms:
Interview the child or adolescent and parents separately and together.
History:
Mental Status Exam – Signs of Depression
| Appearance | disheveled appearance and/or poor hygiene, downcast facies, tearfulness, scars |
| Engagement | poor eye contact, poor engagement/uncooperativeness |
| Behavior | psychomotor agitation or retardation – e.g. slowed movements, few spontaneous movements, distractibility |
| Speech | soft volume, poverty of speech (e.g., brief answers) |
| Thoughts | slowed thinking, perseveration, rumination, guilt- or self-loathing- or self-blame−laden thought content, suicidal thoughts |
| Insight and Judgment | may be poor |
Should include risk assessment for
Suicide Assessment
Use a standardized rating scale.
Columbia-Suicide Severity Rating Scale (CSSRS) – https://cssrs.columbia.edu/the-columbia-scale-c-ssrs/risk-identification/
Assess For:
| Thoughts | active or passive (“I have thoughts about killing myself” v. “I wish I would go to sleep and never wake up”) |
| Plan | methods, date or time |
| Intent | intention to carry out plan |
| Means | ask about firearms, sharps, medications including OTC medications |
Suicide risk assessment culminates in two basic questions:
Screening Tools
Rating Scales
If concern for imminent danger, call 911 or 211, or refer to Urgent Crisis Center or emergency department.
If not imminent risk, call your ACCESS Mental Health for Youth Hub Team for assistance.
Medication Guidelines
How Medication Works
Antidepressants treat depression by restoring inter-synaptic serotonin levels in the brain.
• Monitor weekly for agitation, suicidality, and other side effects.
If at any time the patient displays severe agitation or suicidal ideation with intent or plan, refer to emergency room hospital or crisis team for immediate emergency evaluation.
Consult with ACCESS Mental Health for Youth as needed.
At 4-6 weeks, re-assess symptom severity with PHQ-9
• If score improves < cut-point with mild to no impairment, remain at current dose
• If score fails to improve> cut-point and impairment persists, consider increase or cross-titration to an alternative antidepressant, consult ACCESS Mental Health for Youth for details.
• Monitor successful treatment monthly to assess for relapse, suicidality, and emergent side effects; consult with ACCESS Mental Health for Youth as needed
• Monitor successful treatment bi-monthly during the second four weeks and monthly thereafter for maintenance of remission, to assess for relapse, agitation, suicidality, and emergent other side effects.
For severe agitation or suicidal intent or plan, refer to hospital or crisis team for emergency evaluation; consult with ACCESS Mental Health for Youth as needed.
After 6-12 months of successful treatment, re-assess symptom severity with PHQ-9
• If score < cut-point without impairment, then consider tapering antidepressant medication according to the following schedule: decrease daily dose by 25-50% every 2-4 weeks to starting dose, then discontinue; consult with ACCESS Mental Health as needed.
Tapering should ideally occur during a time of relatively low stress (e.g., summer). Maintenance of antidepressant medication should be considered beyond 6 to 12 months of successful treatment in cases of high severity or risk, recurrent pattern, and/or long duration of illness.
Consider consulting with ACCESS Mental Health for Youth regarding the decision to taper.
Reassess for symptom recurrence with PHQ-9 2-3 months after discontinuation.
Remember that individual responses vary, and it is essential to monitor medication compliance. Parents should always supervise medication administration.
Non-pharmacological Treatment
Triage/Levels of Care
Level of care is determined by two factors: assessment of risk and level of functioning.
To assess risk and safety in depressed individuals, inquire about suicidality and self-injurious behaviors. Intensity (lethality) and frequency will determine level of care.
Outpatient behavioral health services are the least intensive and least restrictive level of care. This entails meeting with a professional therapist or counselor, for a defined period of time such as an hour once a week, and generally provided by appointment in an office setting clinic or virtually. This level of care would be most appropriate for an individual who is experiencing mild to moderate depressive symptoms. This may include infrequent passive SI with no plan or intent and minimal to no history of attempts as well as mild to moderate impact on functioning.
Urgent Outpatient services are for individuals who are not experiencing an emergency but cannot wait for a routine outpatient appointment. This may include an individual experiencing an acute onset of passive or active SI but without any intent or plan and has multiple protective factors (support system, internal coping skills, help seeking and motivation to live).
Resources for urgent mental health care would include, The Village for Families and Children, Yale New Haven Hospital, The Child and Family Agency of Southeastern Connecticut, and Wellmore Behavioral Health. Click here for more information.
Emergency services are available 24 hours per day, 7 days per week, 365 days per year. The purpose of emergency services is to provide a rapid response, assess, and deliver a course of treatment intended to promote recovery, ensure safety, and stabilize the crisis. Emergency services can be provided at locations in the community such as an individual’s home, a PCP office, or local hospital emergency room if necessary. The specific resource for emergency services for children and adolescents are 2-1-1. For more information click here. This may include individuals who are experiencing active SI with plan and/or intent, access to lethal means, and minimal to no protective factors.
Urgent Crisis Centers for Children (ct.gov)
Partial hospital level of care is provided to stabilize acute symptoms, sometimes to prevent an inpatient hospitalization or as a transition between inpatient and home. Partial hospitals provide the same intensity of diagnostic and clinical services but not on a 24-hour basis, usually 6-8 hours per day. This may include individuals who may still have some high risk, however, have been able to demonstrate some level of safety while not in a locked unit (able to utilize supports by communicating needs, able to utilize coping skills, no access to lethal means).
Inpatient hospitalization is the most intensive level of psychiatric care. It is provided in a 24-hour, locked, secure unit within a general hospital or a private psychiatric hospital. Inpatient services are warranted when the child is dangerous to him/herself. This may include depressed individuals who have active SI with plan and/or intent, access to lethal means, and limited to no protective factors.
Residential services vary from short-term acute programs designed to stabilize crises (sometimes referred to as CBAT or Community-Based Acute Treatment) to longer term therapeutic environments that replicate a home-like environment for children who cannot live at home. Residential programs include an educational component arranged with the child’s home-school district. This may include individuals who have treatment resistant depression or those who need longer term treatment in order to reach a level of safety that allows patients to reside at home
Medical Work Up
Psychotherapy
Treating depression in children and adolescents may involve a combination of psychotherapy and medication. For mild to moderate symptoms, psychotherapy alone is an effective treatment for depression.
Psychotherapy is the first line treatment for depression. Selective Serotonin Reuptake Inhibitors (SSRIs) are the first line medication treatment for severe or treatment-resistant cases.
Psychotherapy is an effective intervention for the treatment of depression in children and adolescents. Effective therapy for children and teens involves:
Common therapeutic modalities utilized for the treatment of depression in children and teens are highlighted below:
Cognitive Behavioral Therapy (CBT): an evidence-based treatment that focuses on how thoughts, beliefs, and attitudes affect feelings and actions. Teens and many elementary-age children are able to participate. CBT involves identifying harmful patterns of thinking and implementing step-by-step behavioral changes. The CBT therapist will often give the child or family “homework” in order to help change behaviors and challenge distorted patterns of thinking.
Supportive Therapy: integrates various therapeutic concepts and techniques. Aims to improve, reinforce, and sustain a patient’s physiological well-being or psychological self-esteem and self-reliance. Offering support to depressed children and teens can help them better cope with difficult emotions. The technique often varies from practitioner to practitioner.
Dialectical Behavior Therapy (DBT): a type of CBT that helps people manage their emotions and improve their social relationships. DBT can be most helpful for older children and teens with chronic and intrusive suicidal thoughts and/or self-harm urges. Specialized workbooks and techniques are used to help children understand, accept, and take charge of their thoughts and urges.
Play Therapy: Most commonly used for the treatment of young children who are unable to engage in other therapies. Play therapists will have offices filled with various toys such as doll houses, blocks, cars, puppets, and games. Themes and patterns noted in play, help the therapist and child understand a child’s inner experience and guide how best to express it.
For information on types of therapy used in the treatment of children please see the following resource:
Self-Management Tools
It is also important to guide families and children in lifestyle or behavioral changes while treating depression. These changes can be particularly helpful for more mild forms of depression and can include changes in diet, sleep habits, physical exercise, schoolwork, screen time, as well as time spent together with family and friends. Behavioral activation involves monitoring daily activities can reveal the relationships between activities and mood, identifying a child’s values and goals, and scheduling and carrying out meaningful activities to boost our experiences of pleasure and mastery.
Further guidance can be found at Guided Self-Management Tools for Depression – Parents of Teens 13-17.pdf
Provider Resources
Presentations:
Crisis Link: Urgent Crisis Centers for Children (ct.gov)
AAP Adolescent Depression: Pediatric Mental Health Minute Series: 20-minute educational video https://www.aap.org/en/patient-care/mental-health-minute/adolescent-depression/
AAP’s Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part I. Practice Preparation, Identification, Assessment, and Initial Management https://publications.aap.org/pediatrics/article/141/3/e20174081/37626/Guidelines-for-Adolescent-Depression-in-Primary?autologincheck=redirected
AAPs Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part II. Treatment and Ongoing Management https://publications.aap.org/pediatrics/article/141/3/e20174082/37654/Guidelines-for-Adolescent-Depression-in-Primary
AACAP Practice Parameter for the Assessment and Treatment of Children and Adolescents with Depressive Disorders https://www.jaacap.org/article/S0890-8567(09)62053-0/fulltext
ACCESS Mental Health for Youth Clinical Conversations Trainings
Family Resources
Crisis Link: Urgent Crisis Centers for Children (ct.gov)
AACAP Depression Resource Center – website FAQ for families https://www.aacap.org/AACAP/Families_and_Youth/Resource_Centers/Depression_Resource_Center/Depression_Resource_Center.aspx
AACAP Facts for Families: Depression in Children and Teens –one-page educational handout for families https://www.aacap.org/AACAP/Families_and_Youth/Facts_for_Families/FFF-Guide/The-Depressed-Child-004.aspx#:~:text=Depressed%20adolescents%20may%20use%20alcohol,losing%20someone%20close%20to%20them
AAP Managing Depression or Sadness: Tips for Families: 3-page handout https://downloads.aap.org/AAP/PDF/Family_ManagingDepression.pdf